Changing from the CKD-EPI to the EKFC creatinine equation to estimate glomerular filtration rate in adults in a Northern European health system
Background
The European Kidney Function Consortium (EKFC) 2021 equation to estimate GFR performs as well or better than the CKD-EPI 2009 equation in predominantly white adult European populations, with less bias and greater accuracy against measured GFR. This study explores how changing from the CKD-EPI to the EKFC equation in a large European health system may impact disease distribution, prognosis and clinical decisions.
Methods
We studied over 1.7 million adults in Stockholm undergoing routine care during 2006–2021. We compared eGFR values and reclassification across KDIGO GFR categories when changing from the CKD-EPI to EKFC equation and examined associations of eGFR and reclassification with risk for kidney failure with replacement therapy (KFRT), mortality, and major adverse cardiovascular events (MACE) using Cox models. We also modelled the impact of eGFR equation change on clinical decisions like nephrology referral or medication eligibility/contraindication.
Results
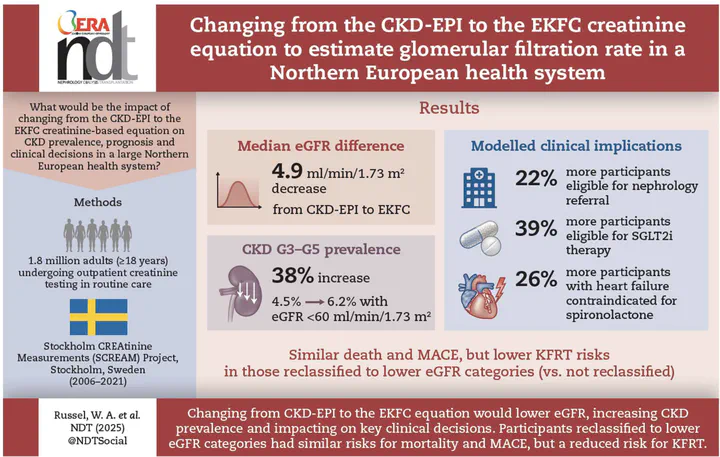
EKFC yielded modestly lower eGFR values than CKD-EPI by a median (IQR) of -4.9 (-8.3 to -2.2) mL/min/1.73m². As a result, CKD G3–G5 prevalence rose from 4.5% to 6.2%. Both equations strongly predicted KFRT, mortality, and MACE. Participants reclassified to lower eGFR categories were older; after adjustment for age, participants had similar risks of mortality and MACE to those not reclassified and a lower risk of KFRT. Changing to the EKFC equation would impact clinical decisions at low eGFR thresholds, such as nephrology referrals (22% higher), eligibility for SGLT2is (39% higher) or contraindication for spironolactone in heart failure (26% higher).
Conclusion
Adopting the EKFC equation in this Northern European health system would modestly lower eGFR estimates, increasing the prevalence of moderate/severe CKD and affecting clinical classification and decisions. eGFR by both equations strongly predicted outcomes, but individuals reclassified to a lower eGFR category by EKFC did not have consistent associations across outcomes.